


FME 4.5 is Like the iPhone X
MARPE is Approaching Maturity

Smash or Pass on MARPE?
Recently a client asked me, “If you were me, would you wait a few more years before taking the plunge on MARPE? Are major improvements coming down the pike?”

I think the answer is: maybe one more year.
If we had a substantial data set of FME before and after CBCT superimpositions, and that data indicated that FME is exactly what it purports to be, I would say the field has matured, and it’s safe to act now.
But we don’t yet.
We have whispers from Dr. Newaz about 50+ FME cases he has done, with just two outright failures to split, and another handful of cases aborted mid-expansion due to other complications.
Overall Dr. Newaz is very bullish on his experience with FME thus far.
But I’ll believe it when I see it.
FME vs. Custom MARPE in 2025
“FME doesn’t always get the split, but when it does, it tends to be an excellent expansion.”
Here I am quoting Dr. Newaz getting to the heart of the FME vs. Custom MARPE debate: Custom MARPE might be better at splitting the suture, but is achieving a split really all that there is to a “successful MARPE case”?
No - it is not. Splitting is not the end-all-be-all. The quality of the split also matters.
Custom MARPE is optimized for getting the split. FME, with its lack of dentally-anchored arms and posterior bias, is optimized for high quality expansion.
These two priorities are in conflict with each other. Sometimes the features that lead to predictable splits are counterproductive to optimal expansion.
For example, placing TADs at the front of the palate with Custom MARPE (where bone is thicker) means less screw drag and screw tipping, but it also means a greater likelihood of more of a Pac-man style, V-shaped, anteriorly-biased expansion which is both less aesthetic and less optimal for nasal breathing enhancement.
Although, to be fair to Custom MARPE, anteriorly-placed TADs don’t entail Pac-man shaped expansion.
To quote Dr. Newaz, “TADs in the front don’t necessarily mean Pac-man. [Rather], the composite of where the whole force system is loaded and the expander behavior (and allowance for said behavior) is what dictates expansion pattern. FME or [Custom] MARPE distributed anterior and posterior and a jackscrew device that doesn’t have the capacity to bow out one way or the other should produce parallel expansion…the FME does this a bit better than the MARPE but both can open evenly.” [Emphasis mine]
A Split is Not a Split
To use an analogy from Dr. Gunson, chocolate cake is not always the same as chocolate cake. A cake baked by a Michelin star chef is not the same as one baked by a 4th grader.
When it comes to MARPE, a split is not a split.
There could be anteriorly biased, asymmetric splits with lots of dental flaring. But they are still technically “splits” that a Custom MARPE provider might count in their high percentage of “successful cases” (success being defined here as getting a diastema).
And then there are nice, parallel splits with zero dental anchorage, with optimal cephalometric pre-planning and high dimensional stability of the appliance that ensures low risk of asymmetry.
Such a clean split and expansion is what ought to be considered a real MARPE success.
Does Everyone Need an FME?
No. Custom MARPE, if customized to act like FME (hence “custom”), can also achieve posteriorly biased, symmetric, purely skeletal expansion.
But if you’re Vegas, you bet on the FME every time, since this is explicitly and unashamedly what it does. If you’re shopping for an EV, do you buy a Tesla or an electrified Ford Mustang?
FME gambles not getting the split in exchange for ensuring that the splits are high quality when they do in fact come.
My job is to advocate for patients both individually (through 1-on-1 coaching) as well as at scale (through no or low cost content like this).
At scale, FME is the safer bet.
Individually, a Custom MARPE with a top provider might still be the better overall option, after logistics (such as geography and cost) are considered.
The New FME 4.5
The new FME 4.5, now being implemented by Dr. Newaz, improves upon the biggest weakness of FME 3.5, namely the lack of obliquely-angled (diagonal) TADs.
In the words of Dr. Newaz, “Oblique engagement increases TAD to bone surface area, and leverages against the tendency of the expander to bend up laterally.”
UPDATED IMAGE OF ACTUAL FME 4.5 (first ever published)


In my recent interview with Dr. Lipkin (set to be published this week on YouTube), he pressed the fact that Custom MARPE is better than FME because of the ability to add obliquely angled TADs, which run more parallel to the palatal bone, and therefore get better anchorage and bend less.
This means more splits, and less failures.

Well, FME 4.5 introduces such oblique TADs. While preserving all of the other features that make it superior to Custom MARPE.
The fight is getting ugly, with top firms stealing each other’s designs. But it’s great for patients!
iPhone X
My sense is that FME 4.5 is like the iPhone X.
Sure, we will get incremental improvements on this design for a decade or two, but the tiny-bezeled, buttonless, flat-piece-of-glass model is basically the end-game of this product.

The next big change will be another paradigm shift, to some kind of VR wearable, or implant, or dictation-centric, AI-governed hardware like the kind OpenAI will likely try to build with Jony Ive.
Similarly with FME, improvements from here-on-out will be incremental, not fundamental. The field is approaching maturity.
With FME 4.5:
Obliquely-angled TADs are used.
Appliance arms are gone.
Symmetry-determining cephalometric analysis is performed by the manufacturer to minimize provider error.
A surgical guide is provided to ensure that orientation errors don’t occur during installation.
The expander body is separate from the anchor body (2-piece design).
TADs lock with threads, to minimize screw wobble.
The use of guide-rods
Protraction is anchored directly to the device (FMA) rather than to molar bands.
I am tempted to say that the time to act on MARPE has arrived, and that safe and predictable expansion is commoditized in the form of FME 4.5.
But I’ve been around the jawhacking space long enough to know that things are not always what they purport to be.
So, my official position is: Dr. Newaz, if you really have 50+ good FME cases that demonstrate that the appliance lives up to the hype, then show us!
We need data. Proof. Once we see that FME is better, rather than just read that it is better, then we can come off the sidelines en masse and play the MARPE field.
Hopefully this occurs within the next year.
Until then, I say proceed with caution on all forms of MARPE and continue to assume the worst. Be moderate with expansion magnitude (4-6mm is a good rule of thumb) and keep a watch out for asymmetry.
Dr. Newaz’s Thesis Statement on FME vs. Custom MARPE
Our position on MARPE and FME isn’t that one is totally better than the other (yet) but that we have different solutions for different situations and we are liking what one of those solutions is offering in terms of expansion quality…I’m a perfect case!
This reads to me a little bit like politically correct fence-sitting, similar to how Dr. Manuele describes his position in the FME vs. Custom MARPE debate.
But my job is to report the facts, and the fact is that the two leading FME providers both state explicitly that they have not yet declared a winner in this fight.
A Note About the Future of this Publication
This Substack was built in 2023 on the premise that I would use it to publish my ebook, Fix Your Face.
Well, I’ve gotten through the first seven parts of that textbook, capped off with this article which brings you to the bleeding edge of MARPE.
The next part of Fix Your Face is on jaw surgery. And I’m not quite ready to write any authoritative texts on that yet.
So, as I continue to learn about orthognathic surgery and conduct more interviews with surgeons, I may treat this Substack more like a traditional newsletter than a textbook.
The content will continue to be cutting edge, just less confined to the linearity of a magnum opus textbook on the entire jawhacking space.
Thanks!
***Originally publushed image referenced in comments by Shuikai and Gandalf
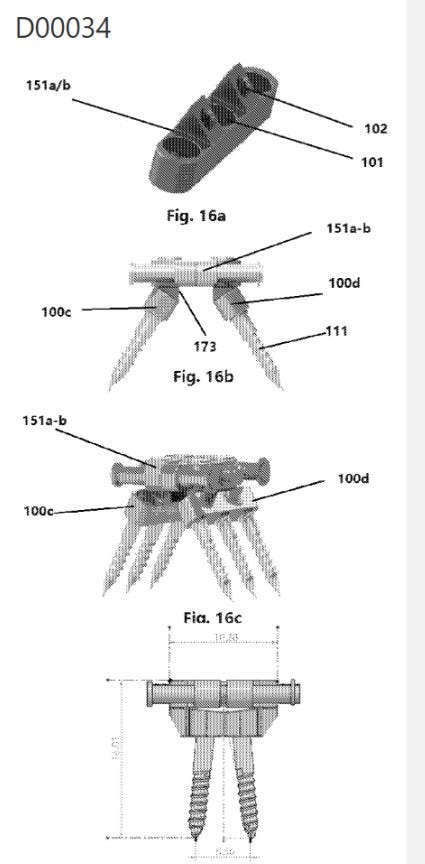
By the way, the picture from that FME patent I believe is from a really long time ago. Definitely not an FME-V or FME 4.5 or anything like that. You'd need to check the dates, but you can see the design of it is even earlier than the 3.5.
I think what Lipkin is saying is that the alveolar TADs provide some stability to the midline TADs, so they are less likely to tip out, because when that happens you get the AGGA effect, dental tipping, etc. With that said, alveolar TADs need to be put anteriorly because the bone there is quite thin in the back. This is why Lipkin's expansions are anterior, unlike MSE or FME.
Are alveolar TADs better? Does it make his MARPE better than FME? Well, that depends on whether or not the FME expands the maxilla DESPITE alveolar TADs. If the TADs aren't bending or tipping out, then you don't need them. If anything, alveolar TADs are a liability from a bone health standpoint. You don't WANT to be pushing on the alveolar bone and applying force there, nor do you WANT to be anchoring to the teeth and applying force there either. Essentially what you are doing with that MARPE design is you are including the patient's biological anatomy as a part of the expander. As both Ron and I are familiar with, when you apply excessive forces to the teeth, alveolar bone, etc. it can lead to bone loss, gum loss, root resorption, etc. Therefore, I would argue that the FME way of doing it is the better option ASSUMING it works without it!
Another point is that I'm sure they could stick some alveolar TADs or molar bands to an FME. They clearly don't want to do that lol.
I did a reverse image search on those FME pics that you uploaded and it looks like they’re from a 2017 patent owned by Facegenics. So, it appears that Facegenics was thinking about the oblique TADs before custom MARPE was even a thing.